
There is much received wisdom on infant sleep and new parents will find that just about everyonethey speak to has an opinion – where, how much, how often. For parents, understanding infant sleep and adapting to new patterns and behaviours can be one of the biggest challenges in the early years. Unsurprisingly, sleep is one of the main concerns presented by parents to paediatricians. By giving parents information about sleep, they can be better prepared to promote and support healthy sleep patterns in their infants. Here is an attempt to decode this mystery.
Understanding Sleep
Understanding the physiological basics of sleep – cycles, patterns, phases and how much we need at different ages – can help health professionals and parents make better sense of infant sleep behaviours. During sleep we all go through cycles of deep and light sleep. An adult’s sleep cycle lasts around 90 minutes, but an infant’s cycle is shorter, lasting 20 to 50 minutes. Deep sleep is quiet sleep; babies are mostly still and breathe evenly, but will sometimes jerk or startle. During light, active sleep, babies look restless, groan, sometimes open their eyes and even wake up completely.
The amount of time we spend in each phase of sleep varies depending on age. Newborns spend about half their sleeping time in a light, active sleep, but by three years old, only one third of sleep time is active. This continues to reduce as children grow older.
For example, frequent night waking can be a problem for some parents but is in fact a normal part of an infant’s sleep cycle. There’s even an argument that night waking serves protective functions by allowing frequent feeding and creating the opportunity for emotional reconnection and brain stimulation. It may be helpful for parents to focus on improving their infant’s ability to self-settle rather than on the frequent waking.
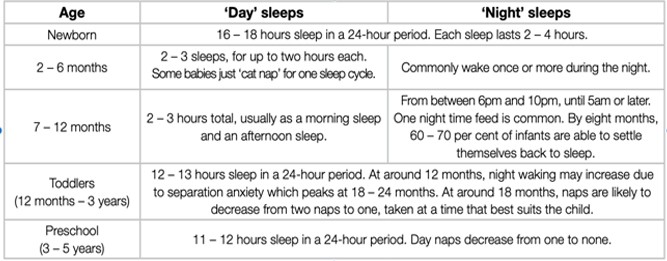
What to expect at different ages?
Each child’s sleep behaviours and patterns will be different. Newborns’ sleep-wake cycles are largely dependent on whether the infant is hungry or full; in older infants, daily rhythms and environmental factors such as light and noise play a much larger role in sleep patterns. As children grow, there is gradual change to their sleep patterns and as these changes occur, it can mean that parents will experience weeks of mixed sleep patterns as children adjust.
Sleep Practices:
Approaches to sleep:
The intuitive parenting position is considered to be based on reading infant behavioural cues and adjusting responsiveness accordingly. This position has an understanding that infant sleep improves over time and that crying will reduce with active comforting strategies. For parents who are interested in following an intuitive parenting style, strategies may include:
- Encouraging parents to use their instincts rather than follow strict rules.
- Trying to interpret the baby’s cries and other cues to understand and respond appropriately to specific needs.
- Providing active comforting including rocking and ‘wearing’ the baby in a sling or pouch.
- ‘Parenting’ the baby to sleep, if required and for as long as the baby needs it.
- Co-sleeping with the baby, including sharing a bed, for as long as needed
Further along the spectrum is the infant behaviour management parenting style. This holds that unsettled infant behaviour is not usually related to illness or otherwise easily explained and because it may cause significant problems for families, it needs to be managed. Parents who are interested in this approach can, after excluding any health-related explanations for the unsettled behaviour, follow active strategies to reduce unsustainable sleep associations and support their baby to learn to settle to sleep.
‘Infant behaviour management’ strategies may include:
- Teachingparents aboutnormalinfantdevelopmental stages and how to recognise and respond to tired cues.
- Separating feeding from sleeping.
- Putting the baby to bed while sleepy, but not yet completely asleep.
- Reducing unsustainable sleep associations such as patting a baby off to sleep. Using rhythmic patting to quieten the baby (but not to the point of sleep).
- Providing the baby with short opportunities to learn to self-soothe.
- Resettling the baby to sleep if s/he wakens after one sleep cycle.
Safe Sleeping
It’s important to acknowledge that while there is no one ‘right’ way for a baby to sleep or be settled, safety should always be the top priority.
Five safe sleeping messages for health professionals from SIDS and Kids:
- Sleep baby on the back from birth, not on the tummy or side.
- Sleep baby with face uncovered (no doonas, pillows, lamb’s wool, bumpers or soft toys).
- Avoid exposing babies to tobacco smoke before and after birth.
- Provide a safe sleeping environment (safe cot, safe mattress, safe bedding).
- Sleep baby in their own safe sleeping environment next to the parent’s bed for the first 6 to 12 months of life i.e. in a cot, bassinet or other separate sleep surface.
Co-sleeping
It is generally advised that parents sleep with their infant in close proximity but on a different sleep surface. The current evidence shows that it is the circumstances in which bed-sharing occurs in sleeping environments that contributes to increased risk of sudden infant death, not the act of bed sharing itself. Nevertheless, it is not safe to share a sleeping surface with a baby if either parent is:
- a smoker
- under the influence of drugs that cause sedation or alcohol
- excessively tired.
It is also not advisable for parents to share their bed if one or both parents are obese.
To avoid the risk of any bedding covering an infant’s face, sleep them in an infant sleeping bag or under lightweight blankets; doonas, pillows and other soft items should be removed from around the baby.
Crying and Sleeping Crying that is difficult to console in the early weeks and months of an infant’s life is part of normal behavioural development. While these early cries can be frustrating, exhausting and demoralising for parents, it can be reassuring to know that it is normal and will pass.

Barr’s crying curve shows that the overall amount of crying per day (fussing, crying and inconsolable crying combined) tends to increase week by week, peak during the second month, and then recede to more stable and lower levels by the fourth or fifth month (Barr, 2006). At its peak, crying lasts on average, around 21⁄2 hours a day , but can be longer in some babies.Other properties that are typical, and probably unique in the first months of life, include crying bouts:
- that are unexpected, unpredictable and unrelated to anything that is going on in the environment
- that are resistant to soothing, or inconsolable
- where the infant appears to be in pain, even when they are not
- that are longer than at any other time, lasting 35 to 40 minutes on average, and sometimes lasting one to two hours or more
- that cluster in the late afternoon and evening.
If you need any further information, you can comment below or call Motherhood Chaitanya Hospital at 0172-5088088, 01762-509503.